It looks like something from a science fiction movie; maybe something from the Alien franchise or Robocop. A console-controlled medical robot with gimbal arms, controller-pods and cameras poised over a surgical table. But this is not a scene from the future. It is the here and now.
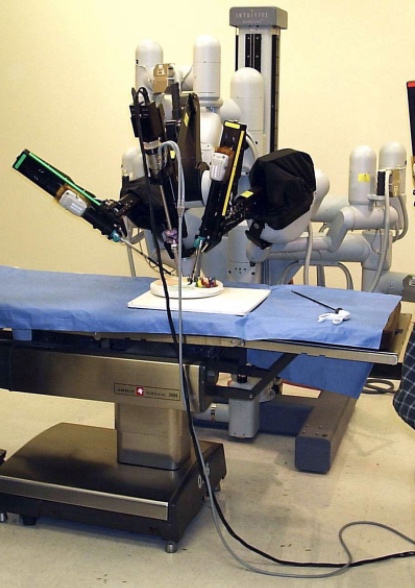
This medical robot is the Da Vinci Surgical System1. It is manufactured by the US company, Intuitive Surgical and is used for gyneacologic surgical procedures.
Robots have been making their entry into the realm of medicine since the 1990s, along with a demand for minimally invasive surgery. Since then, the growth of the robotics industry and the emergence of artificial intelligence (AI) technology have driven advances in robotic surgery.
The system Da Vinci system has a high-resolution 3D vision system that accurately captures images via miniature cameras. When coupled with an advanced motion control system, this allows a surgeon to control Da Vinci’s robotic arms, which can then replicate what the human arm can do; with the capacity to perform complicated surgeries.
Minimises patient downtime and preserves fertility
The need to advance minimally invasive technologies while lowering medical costs is driving the impetus towards robotised surgery (RS). Gyneacological procedures are an obvious choice for robots because of the complexity of the procedures and the confined space for working. As an example of current practice in gyneacological surgery, a team at Rutgers New Jersey Medical School in the US have been using RS to treat endometriosis. Professor Peter McGovern is leading the team and reports minimal downtime for the patient and a better chance of preserving fertility.
For the RS procedure, using a Da Vinci medical robot, multiple robotic arms are inserted into several small incisions, which allows surgeons to see, access and work in nearly the entire pelvic area. Professor McGovern said, “We use robotic surgery for advanced endometriosis cases or subsequent surgeries because it allows for greater articulation of movement and increased dexterity. The enhanced visibility and precision also allow surgeons to work in very small spaces while reducing the risk of damage to pelvic structures.”
Use of RS has seen improvements in:
- Recovery time: Patients recover quickly, particularly if they have had open surgery before for another condition
- Use of opioids: Smaller incisions minimise the need for opioid painkillers and other non-opioid methods of pain control can be used
- Fertility preservation outcomes: use of RS allows the team to implement a fertility-directed approach to surgery leading to better fertility outcomes.
On this last point Professor McGovern said, “I can treat endometriosis with minimal damage to the uterus and I can almost always preserve the ovary, even when removing a cyst. After the cyst is removed, the robot allows me to use a fine suture to close the ovary, which minimizes bleeding and scar tissue.”
The drawbacks of RS
The main issue at the moment is not necessarily one of optics or manipulation of tissue with robotic arms, surgical instruments and tools, although there are real opportunities to vastly improve in these areas in the next few decades. The problem is the lack of force-feedback, the feel of tissue resistance that is essential to inform the surgeon’s precise actions. The solution to this problem is data driven. It requires putting in the long-term work of building databases on physical characteristics of patients, particularly the interaction between human soft tissues and surgical instruments and data on calibrations of the operator-instrument interface. It is a case of fine tuning the relationship between the surgeon’s input and the robot’s output in terms of actions.
Precision is another issue
Current RS is an example of a master/slave robotic system where one device, the master, which ultimately is the surgeon has directional control over the other such as the camera/arm/tool. It is likely that new robots will improve on this master/slave situation. For instance, in China, researchers have built a model of bilateral control, enabling simulation of control signals at the master end to ensure their accuracy before they are sent to the slave devices.
In essence this means that each movement of the surgeon could, in future, be interrogated by the robot before it is allowed to proceed, minimising the chance of human error. This is, of course, another benefit of RS as it evolves alongside advancements in machine learning, data analytics, computer vision, and other technologies.
Prohibitive cost
Another drawback is cost, the Da Vinci Surgical System costs about £1.7 million, with maintenance costs at around £100,000 per annum. However, some insurance companies will cover the cost of procedures using robotic surgery. The system is currently used mainly in private practice with a typical hysterectomy costing the patient around £12,000.
It is interesting to speculate on where this could all take us by the end of the century. If you considers how much, say, a new technology such as medical imaging changed from the 1920s to the year 2000 – from basic X-Rays to positron emission tomography you could argue that all surgery will be robotized in some way or form by the end of the century.
References

